DACRYOCYSTORHINOSTOMY – DCR
Dacryocystorhinostomy (DCR) is a surgical procedure that aims to eliminate fluid and mucus retention within the lacrimal sac, and to increase tear drainage for relief of Epiphora (tears running down the face).
A DCR procedure involves removal of bone adjacent to the nasolacrimal sac and incorporating the lacrimal sac with the lateral nasal mucosa in order to bypass the nasolacrimal duct obstruction. This allows tears to drain directly into the nasal cavity from the canaliculi via a new low-resistance pathway.
DCR treats Nasolacrimal Duct Obstruction (NLDO), a disease that can result in a watery eye, due to obstruction of the outflow of tears, which can have Symptoms including;
• Tearing (Epiphora)
• Mucopurulent discharge
• Matting of lashes and lids, crusting in the morning
• Persistent Pain
• Blurred vision from tears
• Bloody tears
• Dacryocystitis (abscess infection of lacrimal sac in inner corner of eye)
Primary Surgical DCR Options:
1. Primary External Dacryocystorhinostomy
A large osteotomy is created with direct visualization of lacrimal sac abnormalities, such as lacrimal stones, foreign bodies, or tumors. Direct suturing of the nasolacrimal sac and lateral nasal mucosal flaps allow for optimal apposition and primary intention healing of the flaps to create the bypass system.
Advantages of the external DCR approach include excellent success rates, reported to be up to 90% to 95%.
2. Primary Endonasal Endoscopic Assisted Dacryocystorhinostomy
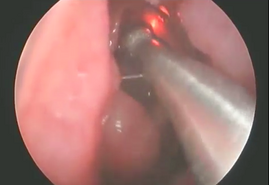
A nasal endoscope is used for visualization. Under endoscopic view, the lateral nasal mucosa adjacent to the lacrimal sac is incised and elevated. A fiberoptic endoilluminator, may be inserted through the canaliculi into the sac in order to help transilluminate the lacrimal bone medial to the lacrimal sac if needed. The lacrimal bone is removed with a drill, rongeurs, or lasers to create an ostium.
Advantages of the internal, or endonasal, approach include lack of a skin incision. Success rates are typicaly reported to be in the range of 85% to 90%.
Overview of DCR Surgical Techniques
Anesthesia: Both forms of DCR surgery may be performed under monitored sedation or general anesthesia based on the surgeon and patient’s preference. The patient may typically be discharged home on the same day.
Local anesthesia, using an equal mixture of 1-2% lidocaine and 0.5% bupivicaine, with 1:100,000 epinephrine, is infiltrated into the medial canthus, lower lid incision site, and nasal mucosa.
Nasal packing soaked in 4% cocaine, lidocaine, or afrin (oxymetazoline) provides additional nasal anesthesia and mucosal vasoconstriction to the middle meatus. Meticulous hemostasis is crucial to a successful DCR surgery.
Technique (External DCR): A curvilinear skin incision is made with a surgical marking pen at the level of the medial canthal tendon and extending into the thin skin of the lower lid for approximately 10-12 mm. The patient’s face is prepped and draped in the usual sterile fashion. A lubricated corneal protective lens is often placed on the ocular surface to protect the globe during surgery.
The skin is incised with a 15-blade scalpel or monopolar unit with a Colorado needle tip. The orbicularis oculi muscle fibers are separated until the periosteum of the anterior lacrimal crest is identified. The dissection should be lateral to the angular vessels to avoid bleeding. The periosteum along the anterior lacrimal crest is next incised from the level of the medial canthal tendon extending inferiorly, and the periosteum widely elevated with Freer elevators anteriorly off the nasal bone. The periorbita and lacrimal sac are similarly elevated posterolaterally off the lacrimal sac fossa. The fossa is next carefully perforated where the bone thins at the suture line between the thicker frontal process of the maxilla and the adjacent thinner lacrimal bone.
Kerrison rongeurs or a high-speed drill are used to remove the bone of the lacrimal fossa, inferiorly to the lacrimal duct at the inferior orbital rim, and anteriorly past the anterior lacrimal crest. A bony ostium measuring approximately 15mm is removed, taking care to avoid a cerebrospinal fluid leak or injuring the underlying nasal mucosa.
A 0-0 Bowman probe is passed into the lacrimal sac to tent the sac medially, and Westcott scissors are used to open the lacrimal sac from the duct to the fundus, with relaxing incisions at both ends. Any abnormal scar overlying the opening of the common canaliculus, lacrimal sac stones, foreign bodies, or masses are removed if present. A corresponding incision is made in the nasal mucosa, to create anterior only, or anterior and posterior flaps.
Lacrimal sac opened to create a flap, and a corresponding nasal mucosal flap is elevated. The lacrimal sac flaps are meticulously anastamosed to the nasal mucosal flaps after silicone tubes are passed into the canaliculi and through the DCR ostium.
The silicone tubes are placed through the new ostium and the flaps sutured together.
After suturing the flaps together to create the new pathway into the nose, the orbicularis muscle and skin are closed in layered fashion. The anterior limb of the medial canthal tendon is also resuspended if released earlier. The silicone tubes are tied and left long in the nasal vestibule to facilitate office removal later. The tubes are typically removed anywhere from 4 weeks to several months after surgery.
Technique (Endonasal/Endoscopic DCR): The primary benefit of the endonasal, or internal, approach is the lack of skin scarring. The nasal mucosa and middle turbinate are first decongested for vasoconstriction and hemostasis.
Using a nasal endoscope for visualization, the lateral nasal mucosa adjacent to the lacrimal sac is then incised vertically and elevated. The sac location is typically located anterior to the anterior aspect of the middle turbinate along the nasal wall.
A fiberoptic endoilluminator, as used in vitreoretinal surgery, may be inserted through the canaliculi into the sac in order to help transilluminate the lacrimal bone medial to the lacrimal sac if needed. Location of the lacrimal sac, anterior to the middle turbinate, is also often confirmed using transillumination.
Full exposure of the bone adjacent to the lacrimal sac is needed. Wide elevation of the nasal mucosa is performed with Freer elevators, and the mucosa removed with endoscopic forceps.
The lacrimal bone is next removed with a high-speed drill, Kerrison rongeurs, pituitary rongeurs or high powered. The final bony ostium should be approximately 8 mm in height and include adequate clearance of the common canaliculus internal ostium and the inferior sac to avoid persistent accumulation in the inferior sac (lacrimal sump).
After bone removal, the lacrimal sac mucosa is infiltrated with local anesthetic for vasoconstriction, incised, and the medial sac mucosa removed with forceps. Adequate lacrimal sac mucosal removal is confirmed by free flow of saline or fluorescein from the canaliculi through the nasal ostium, or direct visualization of the common internal punctum with the endoscope.
Bicanalicular silicone intubation may also be placed as in the external DCR approach, and removed postoperatively in the office. Mitomycin C, an antimetabolite, may judiciously be applied to the intranasal ostium to modulate fibrosis.
The endonasal DCR is contraindicated for patients with a suspected lacrimal system neoplasm, or lacrimal sac diverticulae, lacrimal system stones, common canalicular stenosis, and severe midfacial trauma.